1. Diagnostic basis.
The diagnosis of breast cancer includes four aspects: symptoms, laboratory examination, imaging examination and pathological diagnosis.
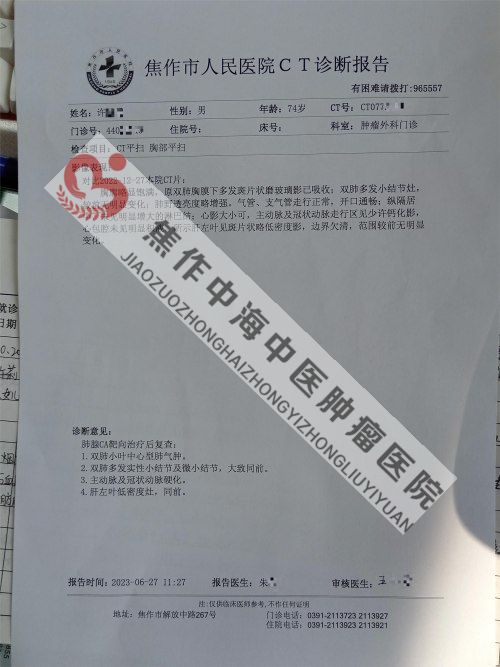
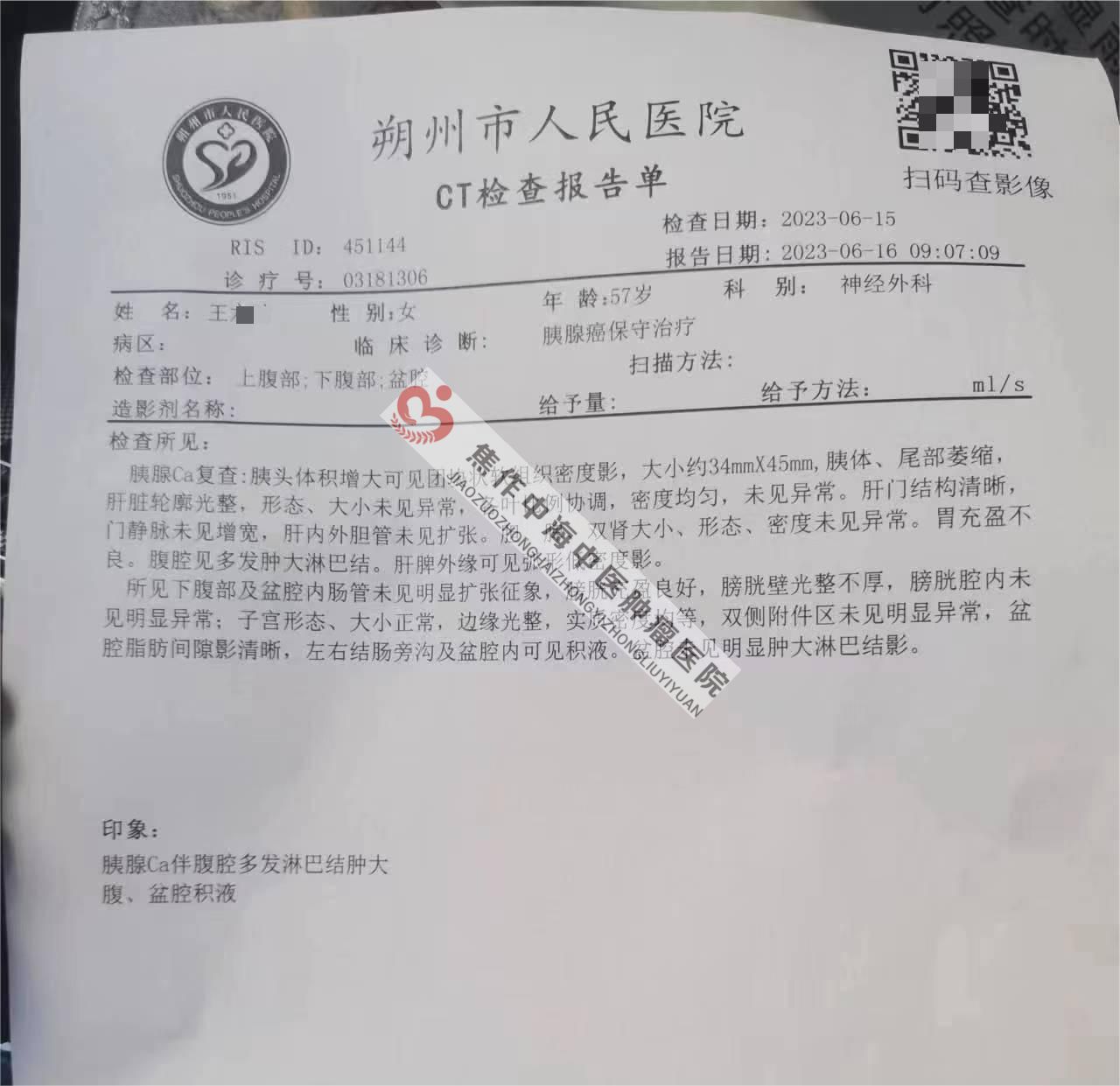
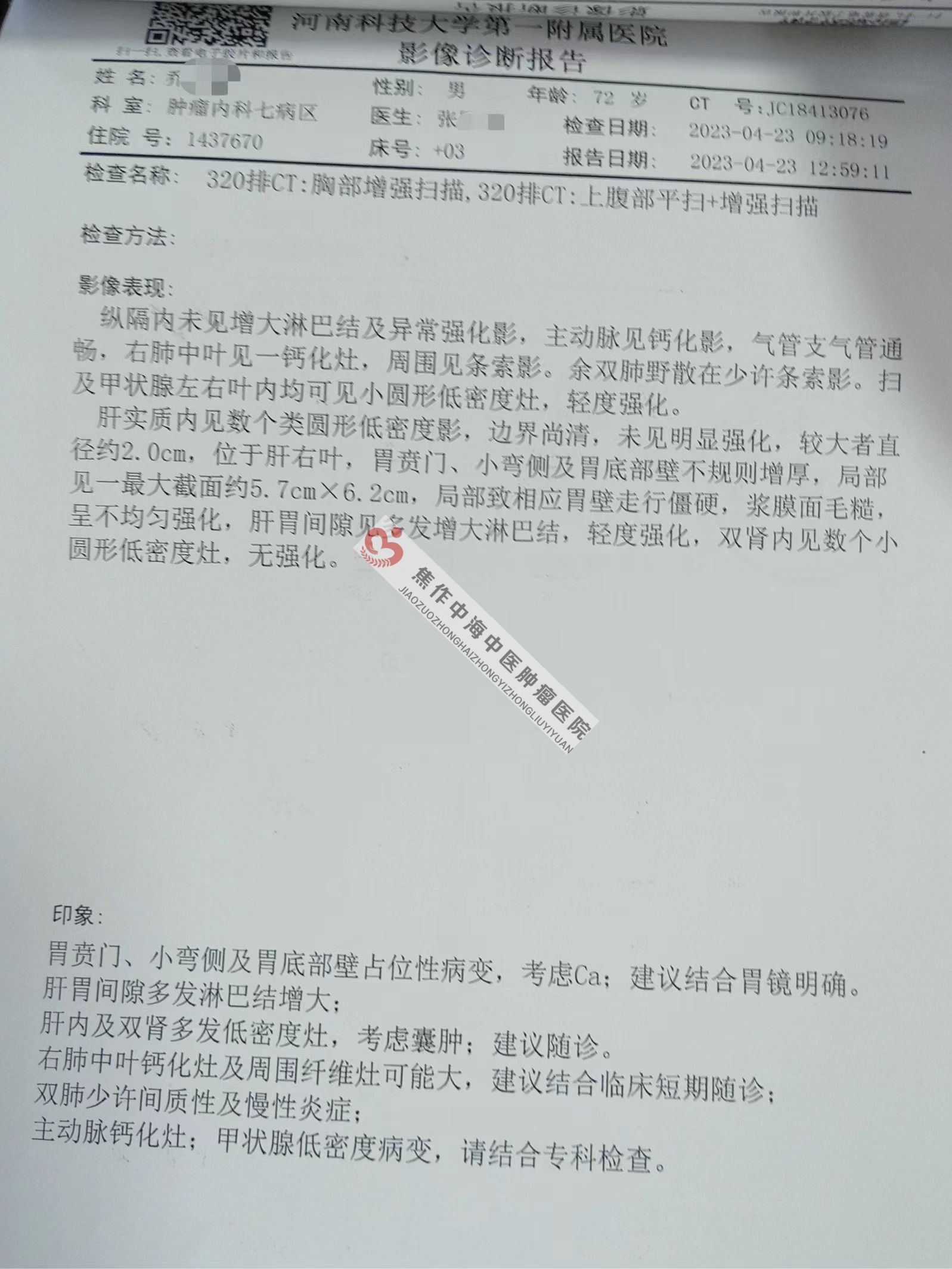
1. Symptom diagnosis.(1) Local symptoms:There may be breast masses, sunken skin (dimple sign), "tangerine peel-like" changes, flat, retracted, sunken nipples, and bloody nipple discharge.(2) enlarged regional lymph nodes:Often the axillary lymph nodes on the affected side are enlarged, hard, painless, and can be pushed; after that, the number increases, fuses into a mass, and even adheres to the skin or deep tissue.(3) systemic symptoms:There are generally no systemic symptoms in the early stage and metastatic manifestations in the late stage, such as chest pain, cough, hemoptysis and shortness of breath during lung metastasis; low back pain and pathological fracture during bone metastasis; hepatomegaly and jaundice during liver metastasis.(4) Special breast cancer manifestations.1) inflammatory breast cancer:It is rare and usually occurs in young women, especially during pregnancy and lactation. The performance is breast enlargement, rapid development, skin redness, heat and pain, like acute inflammation; palpation of the whole breast swollen and stiff. The metastasis is early and the prognosis is very poor.2) eczema-like carcinoma of the nipple (also known as Paget's disease):Rare, low degree of malignancy, slow development. Performance: nipple itching, burning, eczema-like changes, followed by nipple areola rough erosion, desquamation, such as eczema, and then the formation of ulcers. When the lesion develops, the nipple is sunken and damaged. Lymphatic metastasis appeared late.two。. Laboratory diagnostics:Blood CEA and CA153 can be increased.3. Imaging diagnosis.(1) X-ray mammography:It is an important method for the diagnosis of breast cancer, with a detection rate of 30% ~ 50%. It is characterized by localized dense infiltration, burr and malignant calcification. However, young patients may be false negative, and small cancer foci close to the chest wall are easy to be missed.(2) Ultrasonography:Ultrasound images of breast cancer can show. 1 shape and size of the mass; 2 internal echo; 3 calcification; 4 local blood flow imaging; 5. It can be detected when axillary lymph nodes are enlarged.(3) CT check:It can clearly show the mass and calcification in the breast tissue, and can also show the enlargement of axillary lymph nodes and the invasion of chest wall muscle.(4) MRI check:It can be used for staging evaluation to determine the extent of ipsilateral breast tumor, the presence of multifocal or multicentric tumors, or to screen contralateral breast tumors at initial diagnosis.(5) whole body screening:In addition to the examination of the primary tumor, the whole body should be screened before treatment (especially those preparing for surgery) to determine whether there is metastasis and the degree of metastasis. The screening methods include ultrasound, CT, MRI, ECT and PET/CT.4. Pathological diagnosis:Needle aspiration or biopsy is the most accurate basis for the diagnosis of breast cancer. Pathological diagnosis of breast cancer includes histology.Type, pathological grade and on this basis. The hormone receptor and HER-2 were detected on the.(1) histological types.1) carcinoma in situ:Non-special type, lobular carcinoma in situ, ductal carcinoma in situ, Paget's disease with ductal carcinoma in situ.2) invasive carcinoma:Non-special type, ductal carcinoma, inflammatory carcinoma, medullary carcinoma (non-special type), medullary carcinoma with lymphocytes, mucinous adenocarcinoma, papillary carcinoma (dominated by micropapillary carcinoma), ductal carcinoma, lobular carcinoma, Paget's disease with invasive carcinoma, unpulverized carcinoma, squamous cell carcinoma, adenoid cystic carcinoma, secretory carcinoma, cribriform carcinoma.(2) histopathological grading:All invasive breast cancer (except medullary carcinoma) should be graded (G). The grade of the tumor is determined by the morphological characteristics (including the degree of glandular duct formation, nuclear pleomorphism and mitotic count). The score of each item ranged from 1 (good) to 3 (poor). Then the three kinds of scores were added together, and three grades were divided into three grades: 3-5 points as 1 grade, 6-7 points as 2 grades, 8-9 scores as 3 grades.GX: unable to judge the degree of differentiation.G1: the comprehensive score is low (good prognosis).G2: the comprehensive score is moderate (moderate prognosis).G3: the comprehensive score is high (poor prognosis).(3) hormone receptor and HER-2 detection:Breast cancer-related hormone receptors include estrogen receptor (ER), progesterone receptor (PR), and human epidermis.Long factor receptor 2 (HER-2).5. Risk rating:St.Gallen suggested that postoperative breast cancer can be classified according to tumor response to endocrine therapy and other indicators.Low risk, moderate risk and high risk.(1) low risk:The axillary lymph nodes were negative and had all the following characteristics: pT ≤ 2cm, pathological grade 1, no invasion of peripheral blood vessels of the tumor, positive ER or PR, negative HER-2, and age ≥ 35 years old.(2) moderate risk.1) axillary lymph nodes were negative and had at least one of the following characteristics: pT > 2cm, pathological grade 2 ~ 3, vascular invasion around the tumor, HER- 2 positive, age < 35 years old.2) 1 ~ 3 lymph node metastases and negative HER- 2.(3) High risk:1 1 ~ 3 axillary lymph nodes and HER- 2 positive, 2 axillary lymph nodes > 3.6. Menopausal criteria.Menopause is usually the permanent termination of physiological menstruation. The definition of menopause can refer to the following criteria: after bilateral ovariectomy; age ≥ 60 years; age < 60 years old, and menopause for more than one year without chemotherapy, tamoxifen, Toremifene and ovarian function inhibition therapy. At the same time, blood follicle stimulating hormone (FSH) and estradiol (E2) levels are within the range of postmenopausal women. However, menopausal patients under 60 years old who are taking tamoxifen and Toremifene must continuously detect their blood FSH and E2 levels in accordance with the postmenopausal range.7. Clinical staging.Primary tumor (T): clinical (cT) and pathology (pT) adopt the same T classification criteria. If the size of the tumor is determined by physical examination, it can be expressed as T1, T2 or T3. If it is obtained by other measurement methods, such as mammography or pathological measurement, then the subclassification of T1 can be used. The measurement should be accurate to millimeters. For those slightly exceeding the critical value of T classification, such as 1.1mm or 2.01cm, it can be recorded as 1
2. The basis of treatment

1. Surgical treatment.
Surgery is one of the main treatment methods for breast cancer. there are many surgical treatment methods for breast cancer, including radical mastectomy, extended radical mastectomy, modified radical mastectomy, less than total mastectomy (breast-conserving surgery) and so on, especially breast-conserving surgery. the principle of its application must be strictly grasped.
two。. Radiation therapy.
(1) postoperative radiotherapy:
Radiotherapy after surgery for some breast cancer can reduce the local and regional recurrence rate.
1) it should be carried out in principle after breast conserving surgery.
2) patients with tumor > 5cm and more than 4 axillary lymph node metastases after radical resection.
3) patients with 1 ~ 3 axillary lymph node metastases can also be treated with postoperative radiotherapy.
(2) preoperative radiotherapy.
The main results are as follows: 1) the primary focus is large and it is difficult for direct operation.
2) the tumor grows rapidly and increases obviously in a short time.
3) obvious skin edema or chest muscle adhesion in the primary focus.
4) those with large axillary lymph nodes or obvious adhesion with the skin and surrounding tissues. However, the shortcomings of preoperative radiotherapy include increasing operative complications, affecting the correct postoperative staging and the determination of hormone receptors.
(3) radiotherapy of recurrence and metastasis: when local recurrence occurs after operation, appropriate local radiotherapy can improve the quality of life and prolong survival time, and wide field irradiation should be used as far as possible. Distant metastasis of breast cancer can be combined with radiotherapy to relieve symptoms, such as bone metastasis patients can reduce or disappear pain, but also prevent or delay the occurrence of paraplegia caused by thoracic and lumbar metastasis.
3 chemotherapy.
(1) Neoadjuvant chemotherapy:
Neoadjuvant chemotherapy is a routine therapy for patients with locally advanced breast cancer, which can reduce the size of the tumor, reduce the scope and trauma of operation, and make some untreatable tumors can be cured by operation and reduce micrometastasis during operation. All effective chemotherapy drugs and regimens for breast cancer can be used as neoadjuvant chemotherapy regimens. Neoadjuvant chemotherapy is suitable for 3 ~ 4 cycles.
(2) adjuvant chemotherapy:
After breast cancer operation, adjuvant chemotherapy should be considered except for early patients (PT1mi, PT1a, hormone receptor positive, HER-2 negative). Chemotherapy can be selected according to risk.
1) hormone-dependent patients with negative lymph nodes can choose AC/CE [doxorubicin (epirubicin) / cyclophosphamide] or TC (docetaxel / cyclophosphamide).
2) the triple negative patients with negative lymph nodes can choose FAC (FEC) or AC- T.
3) HER-2 positive patients can choose AC-TH (trastuzumab) or TCH.
4) patients with negative HER-2 and positive axillary lymph nodes (medium and high risk of St.Gallen) can choose two cycles of AC- (docetaxel, 3 cycles), FECx3 Tx3, TAC (docetaxel / doxorubicin / cyclophosphamide), or dose intensive chemotherapy (doxorubicin / cyclophosphamide)-dense paclitaxel.
(3) the principle of chemotherapy for recurrent and metastatic breast cancer.
1) patients with adjuvant therapy who only use endocrine therapy without chemotherapy can choose CMF (CTX/MTX/5-FU) or CAF (CTX/ADM/5-FU) or AC (ADM/CTX) regimen, which is not common in clinic.
2) AT regimen is the first choice for patients who have not used anthracycline and yew chemotherapy, such as patients with failed CMF adjuvant therapy, and AT regimen can also be used in some adjuvant therapy patients who have used anthracycline and / or taxus chemotherapy, but the clinical resistance and treatment failure can also be used.
3) for patients with failed anthracycline adjuvant therapy, the recommended combination chemotherapy regimens are XT (capecitabine plus docetaxel) and GT (gemcitabine plus paclitaxel).
4) for patients with failed taxus treatment, there is no standard regimen recommended at present, and the drugs that can be considered are capecitabine, vinorelbine, gemcitabine and platinum, which should be treated with single drug or combined chemotherapy.